

Abstract
Three-dimensional digital technologies and artificial intelligence (AI) are one of the most recent and relevant advancements in the field of dentistry, including in orthodontics. These systems have enabled clinicians to increase the accuracy of diagnosis and treatment planning, to improve patient care along with reducing treatment planning time.
The present study aims to explore possible applications of the artificial intelligence (AI) to examine the upper airway and to assess the reliability of the automatic evaluation of cone-beam computed tomography (CBCT).
Thirty CBCTs, with the field of view 15*15, were uploaded to the Diagnocat (LLC Diagnocat, Moscow, Russia) account, and the radiologic orthodontic report of each was generated as the basis of automatic evaluation. The same CBCTs were manually evaluated by independent evaluator. 3D color visualization of upper airway, total and minimum volume, UPW, LPW, PASmin and A/N ratio were assessed. The data were collected to allow statistical analysis with Microsoft Excel software. A total of 60 reports were created for 30 CBCTs.
Reliability the correspondence between the two methods was 93.3%. A positive correlation between the minimum sagittal linear dimension (MSLD) on 2-dimensional reconstructed lateral cephalograms and minimum cross-sectional area (MCSA) on the CBCTs and a negative correlation between A/N ratio and total area airway were established.
The AI system can be helpful as an initial evaluation of upper airway screening CBCTs, giving appropriate credibility reports and suggesting additional diagnostic methods for more accurate evaluation if needed. The AI technology can also help improve the accuracy of diagnoses for orthodontic treatment, therefore, helping orthodontists work more efficiently. However, the AI has shortcomings in assessing adenoid hypertrophy (AH).
In conclusion, the fields of artificial intelligence in orthodontic diagnostics can be useful for upper airway screening and also have great priorities. Research in the field of upper airway diagnostics using artificial intelligence requires further studies.
Introduction
Physiological breathing is often affected by anatomic or functional problems, causing the respiratory cycle to be initiated not only through the nose but also through the mouth.1,2,3 Normal breathing is important for normal occlusion and craniofacial development4. It has been proved by the authors of many studies that adenoids lead to chronic oral breathing (OB), and it can cause oromyofunctional disorders, different types of malocclusions.5,6 A normal mode of breathing has been considered important for optimal craniofacial and dental growth and development7. In addition to specific detrimental effects on the facial skeleton, impaired nasal breathing has been reported to cause changes in human head posture8.
Since the type of breathing and the condition of the upper airway affects not only the maxillofacial region, but also the whole organism, it is extremely important to correctly assess the upper airway condition. The first stage – diagnostics is an important key to the correct treatment planning and achieving appropriate results. In fact, not all orthodontists evaluate the upper airway condition before treatment. Many people just don’t know how to do it. Dentists are more focused on cephalometric calculations and data. But if the orthodontist misses important diagnostic information, it makes it difficult to get a good clinical stable result after treatment.
Today in dentistry and radiology there are modern digital technologies that help dentists in diagnostic process. One of such advanced and prospective technologies is artificial intelligence (AI)9. At present, AI has been used vastly in dentistry.10,11,12 Artificial intelligence (AI) is a general term that describes machines that mimic the cognitive functions of human intelligence.13 Currently, AI applications are used in areas such as object detection, image classification. Artificial intelligence can evaluate and analyze cone-beam computed tomography images (CBCTs) and identify different dental pathologies. Also, the technique of artificial intelligence is actively used in orthodontics.14,15 Some artificial intelligence- based programs perform segmentation and visualization of the upper airway.16,27
The aim of this study was to assess the reliability of AI in the automatic upper airway detection on CBCT images.
Materials and methods
This retrospective research was performed following the principles of the Declaration of Helsinki. Thirty diagnostically acceptable CBCTs of patients with various dental anomalies at the age from 9 to 15 years (18 girls and 12 boys) were collected from the private dental clinic, Moscow, Russia. Images were taken from August 2021 to September 2022 and included in the study.
The exclusion criteria were: CBCT with an open mouth, unacceptable quality, containing severe artifacts (motion artifacts), field of view less 15*15, previous orthodontic treatment, severe craniofacial anomalies.
All CBCTs were listed and numbered. Then, all images were uploaded to the Diagnocat software account (DC, Diagnocat LCC, Moscow, Russia), and the radiologic orthodontic report of each was generated as the basis of automatic evaluation. 3D color visualization of upper airway, total and minimum volume were assessed. The same CBCTs were manually evaluated by one independent dentist (evaluator). Using manual image tracing in the WEBCEPH program on reconstructed lateral cephalograms (RLCs), the following parameters were determined and calculated: UPW, LPW, PASmin, A/N ratio.17,18 Table 1 shows the descriptions of the parameters (Table 1).
The evaluator assessed each radiograph independently and separately (without knowing the Diagnocat software evaluation). So first, the evaluator performed a manual tracing of RLCs, determines the PASmin and only after that compared the obtained data from the Diagnocat visualization. As for statistical analysis the mean values of the parameters, the standard deviation and the Pearson correlation were determined in Microsoft Excel 2000.
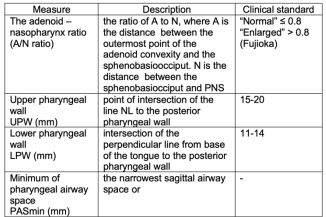
Table 1. Measurements used for 2D airway tracing and analysis.
Results
A total of 30 children were included in the study which consisted of 18 girls (60 %) and 12 boys (40%). Mean age of patients was 11.5±2.45 and most patients were at least 14 years old (9 persons, 30%). All data of both groups was generated in the table (Table 2). Regarding the value of the adenoid index all patients in this study were divided into 2 groups: the first adenoid group with A/N greater than 0.6 (AG) and the second control group less than 0.6 (CG). The AG was diagnosed with adenoid hypertrophy (AH) according to X-ray examination. According to Zhao T et. al the child can be suspected of AH if the A/N ratio is greater than 60%. If the AN ratio is greater than 0.6, a diagnosis of AH will be made.19
In the study of Hamza S. B. et al., an X-ray gradation of the degrees of adenoids was given.20 Adenoid hypotrophy was graded as follows:
- Grade 0 (0.0-0.25) no adenoid enlargement
- Grade 1 (0.26-0.50) minimal enlargement
- Grade 2 (0.51-0.75) moderate enlargement
- Grade 3 (0.76-1.00) gross enlargement.
The results showed that the average of radiologic adenoid size, the radiologic nasopharyngeal size, and A/N ratio for patients of AG were 14.75±2.27 mm, 21.65 ±3.58 mm, and 0.65±0.05, respectively. The average of radiologic adenoid size, the radiologic nasopharyngeal size, and A/N ratio for patients of CG were 14.75±2.27 mm, 21.65 ±3.58 mm, and 0.29±0.1, respectively. The average value of UPW and LPW was 12,7 ±1,9 mm and 9, 8±2,9 mm for the AG. UPW and LPW was 13,7±0,4 mm and 9, 6±0,2 mm for CG. The average value of PASmin 7.25 ±1.2 mm in all patients, 6.75 ±2.6 mm and 7.6 ±2.77 mm for the first and second groups, respectively (Figure1).
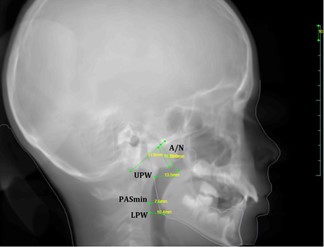
Figure 1. Upper airway measurements on RCLs.
According Hsu W.E et. al minimum of pharyngeal airway space (PASmin) is the most constricted anterior-posterior distance of upper airway, from which a line was traced perpendicular from the posterior wall of the pharynx extending to the anterior wall of the pharynx.21 In our study we also outlined PASmin like the most constricted anterior-posterior distance of upper airway. PASmin is also named like minimum sagittal linear dimension (MSLD) on 2-dimensional RLCs.22 The most frequent localizations of the maximum narrowing of the upper airway in the sagittal direction on RLCs were the oropharynx (63.33%), and then hypopharynx (33.33%). Constrictions in the oropharynx are most often at the level of the uvulae tip and the middle of the soft palate. Regarding the hypopharynx, the constrictions were often at the level of the root of the tongue and the mandibular angle and in some cases below the mandibular angle. In one patient from AG, PASmin was located in the nasopharynx at the level of adenoids.
3D color visualization of the upper airway of 30 CBCT was performed by the Diagnocat program. The artificial intelligence determined the total volume of the upper airway at the level from the upper border (the maxillary plane of the ANS- PNS) to the lower border (epiglottis) and the minimum cross-sectional area (MCSA). The most frequent localizations of the MCSA were the oropharynx (76.6%), and then hypopharynx (40%). The MCSA was less in patients with adenoids.
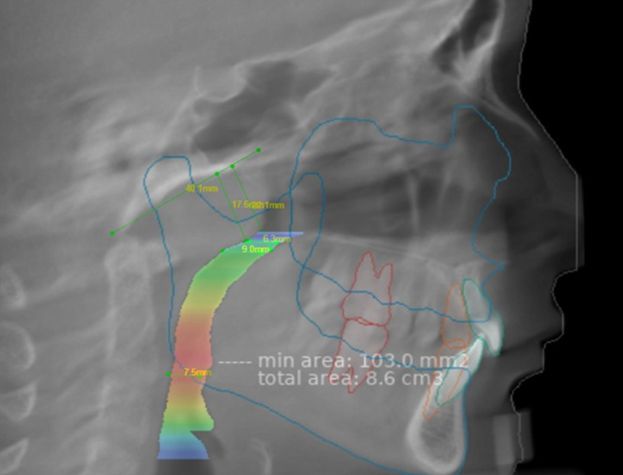
Figure2. The superimposition of automatic and manual upper airway calculation.
The superimposition of automatic and manual calculation of the upper airway was performed (Figure 2). Reliability the correspondence between the two methods was 93.3%. There were 2 special cases. In two patients out of 30 the visualization of the MCSA and PASmin did not coincide. One patient from CG had no adenoids and the AI determined the upper airway volume to the most upper border of the nasopharynx (base of the skull). The MCSA was determined under the base of the sphenoid bone (Figure 3). Another patient from AG had severe adenoid hypertrophy (A/N = 0.83). It was noted that in a patient with grade 2 adenoid hypertrophy, artificial intelligence did not determine the narrowing or presence of pathology in the nasopharynx. The most often the color visualization in the nasopharynx was blue or green, which corresponds to the volume w to a volume of 300-360 cm3, even in patients with adenoids.
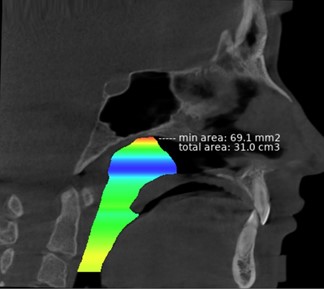
Figure 3. View of 3D color visualization of the pharyngeal airway by Diagnocat.
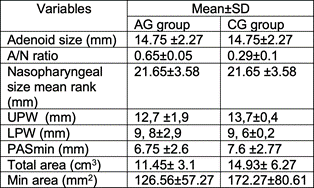
Table 2. Comparison of upper airway measurements between Adenoid Group (AG) and Control Group (CG).
By statistical analysis Pearson correlation coefficient between PASmin and minimum cross- sectional area was 0.289 and 0.338 for AG and CG, respectively. A positive correlation between the MSLD on 2-dimensional reconstructed lateral cephalograms and MCSA on the CBCT scans confirmed the relationship between these parameters. Pearson correlation coefficient between A/N ratio and total area airway was – 0.20 and -0.44 for the first and second group, respectively. A negative correlation between these parameters indicates that an increase in adenoids affects a decrease in the total volume of the airway space.
Discussion
The use of CBCT as a 3D diagnostic tool is increasing because of its advantages over 2D methods.23 Important information obtained from a CBCT scan includes the upper airway assessment, which is essential for treatment planning of patients with adenoids. Previous studies have shown that the upper airway morphology can be studied using 2D and 3D X- ray methods, but CBCT is the most accurate.24,25, 26 Today, the study of the upper airway by means through modern digital technologies and the artificial intelligence are a relevant and prospective direction.
In our study, we tried to evaluate the capabilities of an artificial intelligence-based program Diagnocat in the upper airway assessment in children aged 9-15 years, to clarify CBCT upper airway volumetric assessment, its reliability and limitations, for routine dental clinical use. Computed tomographic measurements of the airway space are not intended to diagnose clinical pathologies, but they have been widely used to screen, assess and monitor treatment outcome.
The automatic protocol for X-ray evaluation by the AI used within this study presented high possibility for the airway space visualization, detection of total and minimum volume. Identifying the location and value of the smallest airway dimension can be useful in screening and planning treatment for patients with adenoids, mouth breathing and other airway space problems.
But low possibility was obtained for adenoid hypertrophy assessment. Diagnocat did not detect moderate or severe adenoid hypertrophy compared to manual 2D assessment of RLCs. The AI did not point out 2 or 3 radiographic degree of adenoid hypertrophy in patients. This important diagnostic information can have critical meaning for treatment planning and obtained results. Positive correlation between MSLD on 2-dimensional RLCs and the MCSA 3-dimensional CBCTs confirmed the clinical reliability of using the method to assess the upper airway.
There are limitations in this study. The evaluated group of 30 CBCTs relatively small, although it provides data for appropriate statistical analysis. The second limitation is the lack of clear guidelines and borders for determining the parameters of the airway space. It is planned to develop new algorithms for AI training. Further researches are needed in this field and authors of this study suggest involving a wider group of evaluators and performing analyses using larger samples.
Conclusions
Within the limitations of this study, we can draw the conclusion that the artificial intelligence application can be helpful for an initial evaluation of screening CBCT for upper airway assessment, except for the definition of adenoid hypertrophy. Moreover, a more complex report generated by this system refers to some potential pathologies to be evaluated by specific specialists and be useful for complex diagnostics and choosing the correct treatment tactics in each individual clinical case.
Declaration of Interest
The authors report no conflict of interest.
References
1. Salem OH, Briss BS, Annino DJ. Nasorespiratory function and craniofacial morphology-a review of the surgical management of the upper airway. Semin Orthod. 2004;10:54-62.
2. Farid MM, Metwalli N. Computed tomographic evaluation of mouth breathers among paediatric patients. Dentomaxillofac Radiol. 2010;39:1-10.
3. Jefferson Y. Mouth breathing: adverse effects on facial growth, health, academics, and behavior. Gen Dent. 2010;58:79-80, 18- 25; quiz 26-7.
4. Faria PT, de Oliveira Ruellas AC, Matsumoto MA, Anselmo- Lima WT, Pereira FC. Dentofacial morphology of mouth breathing children. Braz Dent J. 2002;13(2):129-32.
5. Lessa FC, Enoki C, Feres MF, Valera FC, Lima WT, Matsumoto MA. Breathing mode influence in craniofacial development. Braz J Otorhinolaryngol. 2005;71(2):156-60.
6. Peltomäki T. The effect of mode of breathing on craniofacial growth–revisited. Eur J Orthod 2007;29:426–9.
7. Wang H, Qiao X, Qi S, Zhang X, Li S. Effect of adenoid hypertrophy on the upper airway and craniomaxillofacial region. Transl Pediatr 2021;10(10):2563-2572.
8. Krakauer, L. H., & Guilherme, A. Relationship between mouth breathing and postural alterations of children: A descriptive analysis. International Journal of Orofacial Myology, 2000;26(1), 13-23.
9. Orhan K, Bayrakdar IS, Ezhov M, Kravtsov A, Özyürek T. Evaluation of artificial intelligence for detecting periapical pathosis on cone-beam computed tomography scans. Int Endod J. 2020;53(5):680-689.
10. Zadrożny Ł, Regulski P, Brus-Sawczuk K, Czajkowska M, Parkanyi L, Ganz S, Mijiritsky E. Artificial Intelligence Application in Assessment of Panoramic Radiographs. Diagnostics (Basel). 2022;12(1):224.
11. Ezhov M, Gusarev M, Golitsyna M, Yates JM, Kushnerev E, Tamimi D, Aksoy S, Shumilov E, Sanders A, Orhan K. Clinically applicable artificial intelligence system for dental diagnosis with CBCT. Sci Rep. 2021;11(1):15006.
12. Ahmed N, Abbasi MS, Zuberi F, Qamar W, Halim MSB, Maqsood A, Alam MK. Artificial Intelligence Techniques: Analysis, Application, and Outcome in Dentistry-A Systematic Review. Biomed Res Int. 2021;2021:9751564.
13. Khanagar SB, Al-Ehaideb A, Maganur PC, Vishwanathaiah S, Patil S, Baeshen HA, Sarode SC, Bhandi S. Developments, application, and performance of artificial intelligence in dentistry
– A systematic review. J Dent Sci. 2021;16(1):508-522. doi: 10.1016/j.jds.2020.06.019.
14. Monill-González A, Rovira-Calatayud L, d’Oliveira NG, Ustrell- Torrent JM. Artificial intelligence in orthodontics: Where are we now? A scoping review. Orthod Craniofac Res. 2021;24 Suppl 2:6-15. doi: 10.1111/ocr.12517.
15. Khanagar SB, Al-Ehaideb A, Vishwanathaiah S, Maganur PC, Patil S, Naik S, Baeshen HA, Sarode SS. Scope and performance of artificial intelligence technology in orthodontic diagnosis, treatment planning, and clinical decision-making – A systematic review. J Dent Sci. 2021;16(1):482-492.
16. Sin Ç, Akkaya N, Aksoy S, Orhan K, Öz U. A deep learning algorithm proposal to automatic pharyngeal airway detection and segmentation on CBCT images. Orthod Craniofac Res. 2021;24 Suppl 2:117-123.
17. McNamara JA Jr: A method of cephalometric evaluation. Am J Orthod 1984;86(6):449–469.
18. Fujioka M, Young LW, Girdany BR. Radiographic evaluation of adenoidal size in children: adenoidal-nasopharyngeal ratio. AJR Am J Roentgenol. 1979;133(3):401-4.
19. Zhao T, Zhou J, Yan J, Cao L, Cao Y, Hua F, He H. Automated Adenoid Hypertrophy Assessment with Lateral Cephalometry in Children Based on Artificial Intelligence. Diagnostics (Basel). 2021;11(8):1386.
20. Sunaina Binth Hamza, Ranjith V. T Assessment of size of adenoid-comparison of adenoidal nasopharyngeal ratio and nasal endoscopy in children with chronic adenoiditis. International Journal of Research in Medical Sciences . Int J Res Med Sci. 2019;7(3):776-781.
21. Hsu WE, Wu TY. Comparison of upper airway measurement by lateral cephalogram in upright position and CBCT in supine position. J Dent Sci. 2019;14(2):185-191.
22. Alwadei AH, Galang-Boquiren MTS, Kusnoto B, Costa Viana MG, Lin EY, Obrez A, Evans CA, Masoud AI. Computerized measurement of the location and value of the minimum sagittal linear dimension of the upper airway on reconstructed lateral cephalograms compared with 3-dimensional values. Am J Orthod Dentofacial Orthop. 2018;154(6):780-787.
23. Obelenis Ryan DP, Bianchi J, Ignácio J, Wolford LM, Gonçalves JR. Cone-beam computed tomography airway measurements: Can we trust them? Am J Orthod Dentofacial Orthop. 2019 Jul;156(1):53-60.
24. Kaur S, Rai S, Kaur M. Comparison of reliability of lateral cephalogram and computed tomography for assessment of airway space. Niger J Clin Pract 2014;17:629-36.
25. Sears CR, Miller AJ, Chang MK, Huang JC, Lee JS. Comparison of pharyngeal airway changes on plain radiography and cone-beam computed tomography after orthognathic surgery. J Oral Maxillofac Surg. 2011;69(11):e385-94.
26. Harun Achmad, Rini Sitanaya, Hans Lesmana, Arni Irawaty Djais, Rosdiana Agustin. Effectiveness of Twin Block Device as Upper Airway Correction in Pediatric Patients with Class II Malocclusion and Its Relationship with Muscle Contraction: A Systematic Review. J Int Dent Med Res. 2022; 15(2): 873-884
27. Kamgang W., Kosyreva T.F., Tuturov N.S., Loginopulo O.V., Abakeliya K., Katbeh I. Prevalence of dental anomalies in children in the central region of Cameroon. Endodontics Today. 2022;20(3):272-276.