Chronic sinusitis is often associated with problems in the upper posterior teeth, especially the first molars, whose roots are located in close proximity to the maxillary sinus.
The patient had been suffering from recurrent sinusitis exacerbations for an extended period. The ENT specialist suspected a dental source of infection in the area of tooth 1.6 and referred the patient for a dental consultation.
Examination and Diagnostics
Clinical examination revealed an old restoration on tooth 1.6 with compromised marginal integrity, as well as caries on the mesial surface.
Percussion testing was mildly positive across the entire right side of the maxilla.
At the time of examination, the patient was undergoing medical treatment for an acute sinusitis flare-up and reported associated complaints of nasal congestion and pain.
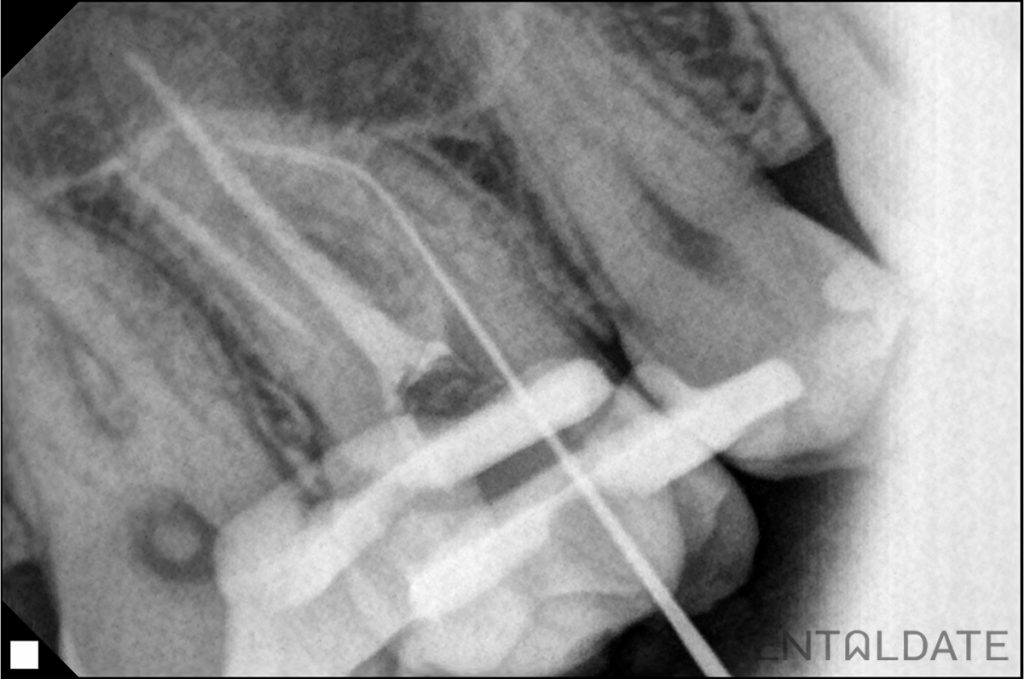
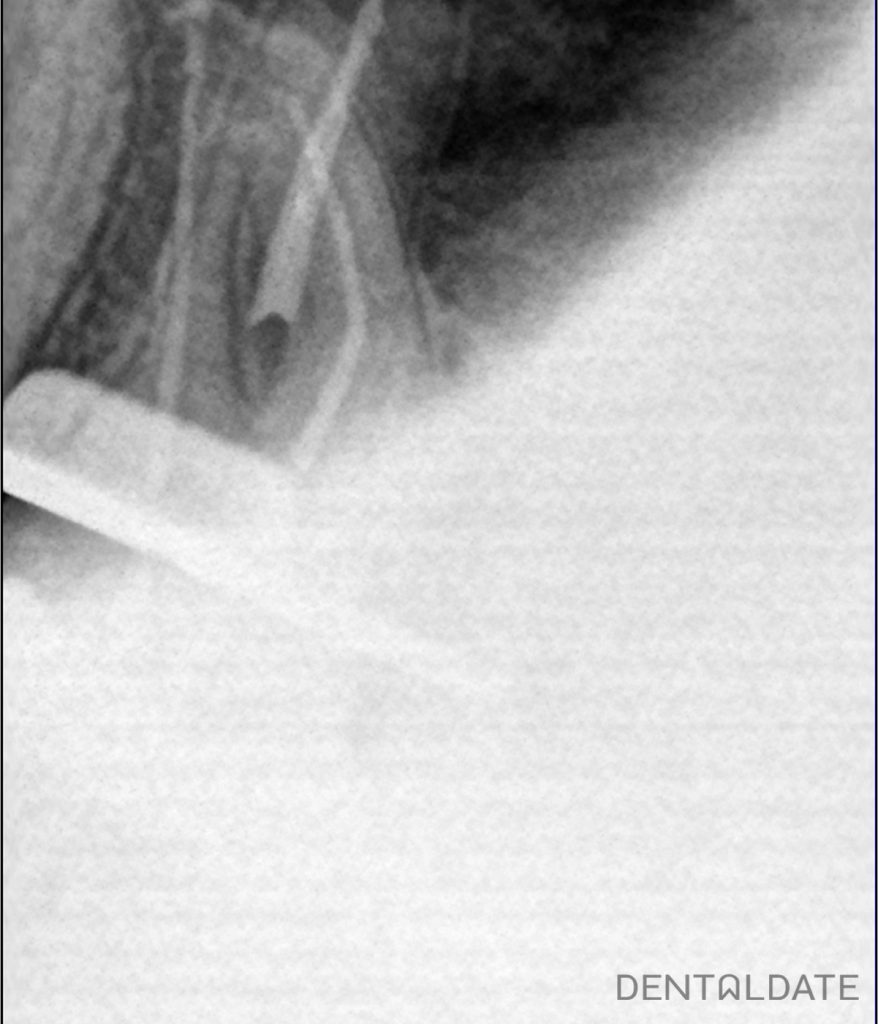
Cone-beam computed tomography (CBCT) findings showed that the tooth had previously undergone endodontic treatment; however, a complex curvature was identified in the apical third of the mesiobuccal root. The root canals were obturated to the apex, but a periapical radiolucent lesion with indistinct borders was visible around the mesiobuccal root apex — a sign of chronic inflammatory pathology.
Treatment Plan
The clinician proposed endodontic retreatment of tooth 1.6 in order to eliminate the source of chronic infection and reduce the risk of sinusitis recurrence.
Treatment Stages
- The old restoration was removed, and a new access cavity to the root canal system was created.
- The canals were carefully de-obturated, taking into account the complex root curvature.
- Calcium hydroxide was placed into the canals for two weeks to achieve disinfection and elimination of bacterial infection.
- After 14 days, the canals were mechanically and chemically prepared and obturated using the warm gutta-percha condensation technique with AH Plus sealer.
- The tooth was restored with a high-quality direct restoration.
- The patient was advised to place a crown on the tooth to protect it from potential fractures in the future.
Treatment Outcome
- The chronic infectious focus responsible for inflammation of the maxillary sinus was eliminated.
- Pain and discomfort in the area of the affected tooth resolved.
- The patient reported an overall improvement in well-being and a reduction of ENT-related symptoms.
- Tooth 1.6 was preserved and is ready for further prosthetic rehabilitation with a crown.
Why This Is Important
Chronic sinusitis often has a dental origin. An infectious lesion at the root apex may sustain sinus inflammation and interfere with effective treatment by an ENT specialist.
Endodontic retreatment under CBCT guidance and with the use of modern materials allows clinicians to:
- preserve a tooth that was previously considered “problematic”;
- eliminate the risk of recurrent sinus infection;
- avoid tooth extraction and more complex surgical interventions.
At DentalDate, a comprehensive approach to such cases has become the standard of care.
We work in close collaboration with ENT specialists, which is particularly important in cases of odontogenic sinusitis. The use of a dental microscope, CBCT imaging, and modern endodontic treatment protocols enables predictable management even of anatomically complex root systems, allowing patients to regain their health without tooth extraction.